Medicare Seeks Savings Beyond Facilities In The Post-Acute Care Continuum
By Jim O’Brien
VP of Partnership Development
Early assessments of bundled or episode-based payment programs suggest that these programs are having a positive material impact on reducing Medicare costs while maintaining equivalent quality outcomes. The objective of the Centers for Medicare and Medicaid Services’ Bundled Payments for Care Improvement Program (BPCI) is to tie acute-care providers to participants in the post-acute continuum by aligning incentives within individual episodes of care.
Physicians operating in today’s higher coordination-of-care environments would benefit from a better understanding of how their downstream care partners impact their quality scores and other factors which influence shared savings initiatives. It is not just the next place of service the patient goes to, but the entire continuum which is critical.
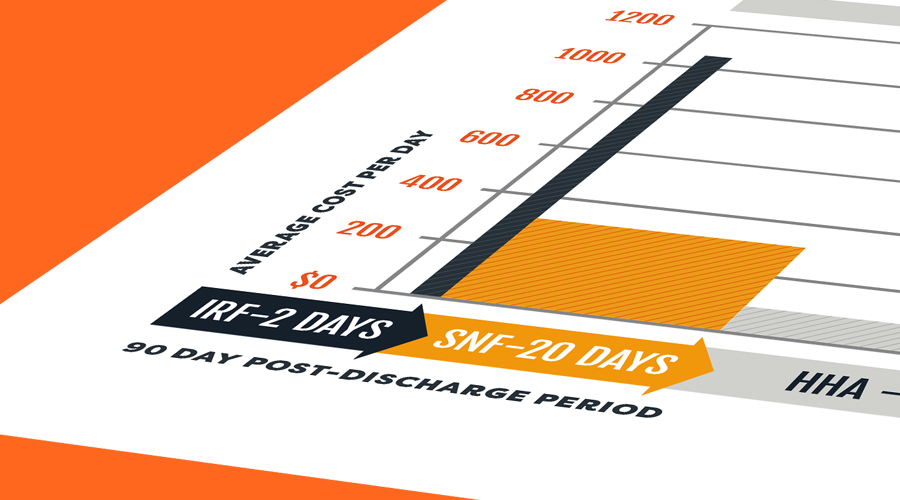
A study in the Journal of American Medical Association from September 2016 showed that Medicare payments declined more for lower-extremity joint replacement episodes provided by BPCI-participating hospitals than hospitals that did not participate over the first 21 months of the initiative. The study detailed how payments declined by an average of $1,166 more for the BPCI population versus the comparable. Savings were primarily achieved through lower Inpatient Rehab Facility payments (IRF spend declined $445 more on average) and lower Skilled Nursing Facility payments (SNF spend declined $546 more on average). This means 85 percent of the differential savings achieved came from squeezing facility-based institutional partners.
The SNF Blueprint
The trend to move patients out of hospital settings began in the 1980s. The result (page 110) was a steady increase in post-acute spending over time. Convener organizations, such as Remedy Partners and PAC Planning Services, identified early on that the next lowest-hanging fruit for bundled payment savings would be found in reducing spend at relatively high-cost SNFs, which generally meant shortening length of stay.
Conveners facilitated the creation of “high-performance SNF networks” which were collections of SNFs that demonstrated the ability to rehabilitate patients more effectively than their peers, creating earlier discharge and shorter lengths of stay. In exchange for shortening lengths of stay, the highest-performing SNFs benefited from increased patient volumes channeled to them from bundle-motivated acute-providers directing patients their way. Lower-performing SNFs saw referral streams dry-up.
One way the high-performing SNFs were able to achieve their shorter length of stays with a minimal impact on clinical outcomes and 90-day re-hospitalization rates was apparently to have tighter partnerships with Home Health Agencies, or HHAs. Specifically, these were HHAs that facilitated patient transitions to the home setting and continued both nursing and therapy services for SNF-discharged patients. The care continuum remained, but beyond the brick and mortar place of service in the lower-cost, home-based place of service.
Beyond the dollars saved by reducing length of stay, the primary measure that post-acute care providers were being held to appeared to be their impact on reducing re-hospitalizations. Hospitals and upstream acute-care providers were being penalized for re-hospitalizations, so they turned up the pressure on their downstream partners, holding patient referral streams out as the carrot to encourage better clinical performance.
Recreating SNFs’ Success
Although HHAs represent a lower-cost alternative to SNFs, they have not been beyond the reach of bundled payment program savings-seekers. HHAs’ length of stay varies dramatically across regions and organizations. This suggests to the conveners of bundles and Accountable Care Organizations, or ACOs, that there is an opportunity to create the same “high-performance networks” that were successful with SNFs.
Physicians who are more conscious of where their patient is headed to next after discharge can have a dramatic impact on both quality outcomes and cost savings. As much as conveners and health systems attempt to create tighter preferred networks, they are only as effective as the individual physicians writing the post-discharge prescriptions for care.
Because HHAs are often reimbursed under the inpatient Medicare Part A benefit, patients do not incur any cost-sharing for home health nursing or therapy visits. While the episode payment is primarily made on a fixed or capitated basis, there are modifiers increasing reimbursement. These modifiers are based on the number of therapy visits a patient received. This dynamic could create a financial incentive to utilize therapy visits as part of the home health plan of care.
CMS has acknowledged this dynamic and is focusing on making changes to reimbursement incentives in some of their reform efforts. One of the current proposals is to do away with the therapy modifier component of traditional Medicare Part A home health reimbursement in 2019. The effect of this change: encourage a shift in therapy place of service from home health to the more cost-effective (page 122) outpatient setting.
Balancing Quality of Care and Costs
These trends appear to demonstrate the continued march toward encouraging patients to receive their necessary care at the most cost-effective place of service. This is assuming there are no negative impacts on the quality of care.
While cost savings are clearly achieved in this process, we must closely monitor the quality of care being delivered. This begins at patient compliance with recommended therapies and ends with clinical outcomes achieved.
Physicians who demand to see outcomes from their post-acute continuum partners (SNFs, Home Health Agencies, and Outpatient Therapy providers will be most effective at ensuring their patients receive high-quality care while still achieving cost savings for the system.