Unlocking the Costochondritis Puzzle

By Jon Keller, PT
One in four older adult Americans will experience a fall each year. Of those, a significant population will suffer rib injuries. A study that analyzed nearly 24,000 patients aged 65 years and older, between 2015-2016, reported the leading cause for rib fracture to be falls (67.6%) Rib injuries can be extremely complicated to treat and take years sometimes to heal properly.
I am 50 years old and 3 years ago I felt a pop in my anterior and lateral rib cage region from hitting a hard first tennis serve. I tried everything to treat it effectively. I went in for 2 CT scans, an Xray, visited several physical therapists, consulted with professors of anatomy and biomechanics in physical therapy, received guided ultrasound injections of cortisone (this helped tremendously for 2 weeks) , had 2 visits with a leading chest wall surgeon at MUSC, tried treatments like heating, icing, myofascial release, cupping, and electrical stimulation, tested every topical medicine available on the market (Voltaren gave relief for about 3 hours), tried medicines from physicians (steroids orally helped significantly for about 1 week…dosing was 10 mg for about 10 days) , tried strengthening, stretching, chiropractic manipulation, tried treating the area above and below the injured area to address the whole kinetic chain of the body, adopted a different diet, and attempted to rest for 2 months. Despite my efforts, I just could not figure out how to fix it. Finally, I received a diagnosis of costochondritis. It was the most baffling and uncomfortable musculoskeletal condition I have seen in 23 years in patients, and the most difficult one to deal with personally.
What is Costochondritis?

Costochondritis is a condition that occurs when some form of trauma is experienced in the front and or side of the rib cage where the cartilage from the sternum meets the ribs. Common examples of the mechanism of injury are swinging a baseball bat, strenuous lifting, a hard tennis serve, severe bouts of coughing, falling on one’s rib cage, and pitching a baseball. Sometimes the pain can be felt right away, but often it shows up several days later. It can show up circumferentially around the whole rib cage and at other times it can manifest as pinpoint pain. The pain can be alarming because it can feel like a panic attack, a heart attack, and or show up as paradoxical breathing. The pain can present in one spot in the ribs, usually in the front, and laterally. It can be in many spots and can periodically improve, then flare up. It can circle around the whole rib cage in a narrow or wide length or width.
Research shows the following trends:
- Age is typically 40+ years old
- Usually more than 1 site of pain (70% of time)
- 2nd to 5th ribs region more commonly sore
- Felt a pop in ribs region
- Pain locally and around whole rib cage usually manifesting itself several days after the initial injury
- No swelling
- Stiffness and/or pain around whole rib cage
- Difficulty breathing
- Can last for many years with little relief and exacerbation episodes
It is difficult to obtain a clear diagnosis because the injury often does not show up on an X-ray, or even a CT scan. I believe this rib condition is under-diagnosed and not treated effectively in the medical community.
Important Biomechanic Considerations
The ribs around the lateral regions move like a bucket handle when we breathe. There are multiple joints to consider for hyper and/or hypomobility. The costosternal joints, the thoracic facet joints, the costotransverse joints, and the costovertebral joints should be assessed. When one inhales the bucket handle (lateral ribs) moves upwards and when one exhales the bucket handle descends. That movement occurs roughly about 22,000 to 23,000 times a day. It is no wonder why the pain is so difficult to get rid of- it is extremely hard to allow this area rest for healing.
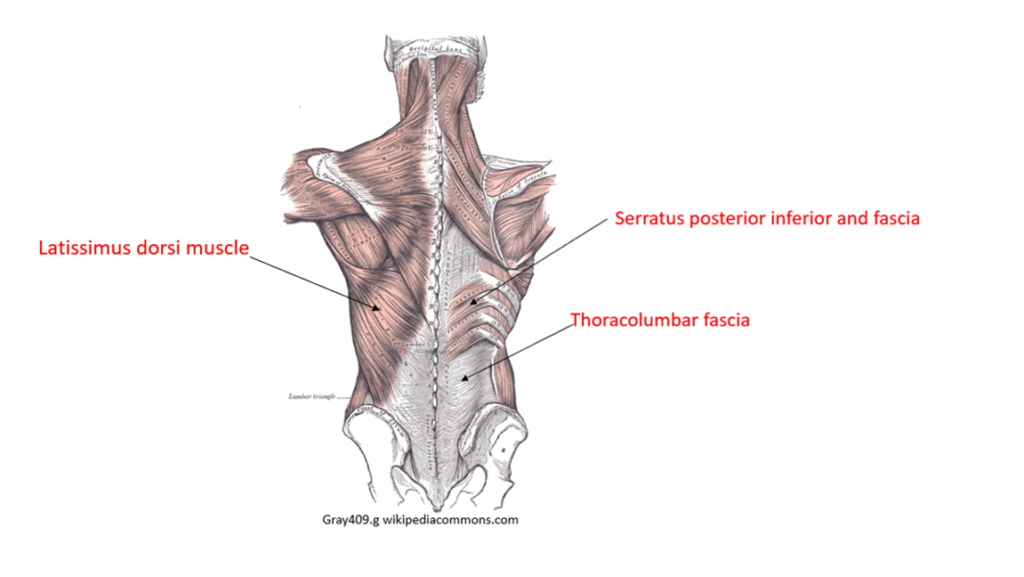
My theory is that the posterior joints, thoracic facet joints, costovertebral, costotransverse joints, the posterior fascia (thoracolumbar fascia, latissimus dorsi/fascia, serratus posterior inferior/fascia) become profoundly stiff and have myriad adhesions with this condition. The anterior rib joints (costosternal joints) thus move excessively and “run hot”. Pain will manifest itself consistently in the front of the ribs and stiffness will be felt in the posterior thoracic region. Another part of the theory is that with the human body, the midback tends to lean forward with bad posture in sitting and standing activities (excess thoracic spine kyphosis.) The sequelae of which is the anterior ribs slide forward/anterior, and the posterior thoracic joint/rib joints slide forward concomitantly.
Differential Diagnosis
- Heart attack
- Pulmonary embolism
- Tietze syndrome (in those younger than 40yrs), usually one pain spot with the 2nd and 3rd ribs more common sites of pain and swelling (treatment basically the same as costochondritis)
- Slipping rib syndrome
- Herpes zoster
- Fibromyalgia
- Neoplasm
- Arthritis at rib joints in sternum or vertebrae
- Painful xyphoid syndrome
- Overuse myalgia (Proulx, et al.)
- Acute thoracic aortic dissection
- Reflux
- Pericarditis
- Pneumonia
- Heart failure
- Panic anxiety attack
- Chest wall pain (Rhim, et al.)
- Rib fracture
Tips to Diagnose
Here are ways to diagnosis it with clinical physical testing corroborated by research.

Crowing rooster maneuvers to attempt recreating or worsening pain associated with costochondritis: Left picture: with patient’s hands clasped behind their head; Right picture: with patient’s arms raised to their sides. With each maneuver, patients are asked to extend their neck (look upward) while the helping party gently lifts the arms superiorly and posteriorly. Reproduction of bilateral costochondral pain will occur. (Mott, et al.)

Crossed-chest adduction maneuver to attempt recreating or worsening pain associated with costochondritis. The patient is asked to turn their head toward one shoulder. Bring the patient’s ipsilateral arm across the chest with gentle, but continuous, pressure. This can be repeated with the opposite shoulder and arm, with the head turned to that side to assess for reproduction of bilateral costochondral pain. (Mott, et al.)
Cause of Chronic Pain
The fascia of the mid back is extremely dense. The latissimus dorsi becomes profoundly tight and stiff very easily with pulling, stabilizing the trunk, and heavy lifting activities. The serratus posterior inferior becomes tight and stiff very easily as well. The thoracolumbar fascia (TLC) has a wide surface area of fascia that connects to these areas. It becomes bound down to bone and muscles.
A side note possibility of chronic inflammation for this region…With chronic inflammation of fascia in the back (TLC) area pain receptors increased from 4 to 15% (Sinhorim, et al.)
- This condition will become reinjured with the slightest of forces or activities… like a “hair pin trigger” (August, Steve)
- Do all you can for 2 months to not reactivate or set off the inflammation process
The symptoms likely will be delayed a day or two from the activity. Common aggravating activities are… Sawing, pulling heavy objects, lifting heavy objects out in front of yourself, dips at the gym, bench press, latissimus dorsi pulls at gym, plank, and sleeping on the sore side (lying supine on back is the best position to sleep)
Any time you reaggravate your symptoms you restart the inflammation process. Sometimes even performing the below exercises can aggravate symptoms. Reducing inflammation is crucial. More scar tissue and adhesions develop. Don’t cause reaggravation of your symptoms!

(Laumonier, et al.)
Effective Treatment Strategies
There is a paucity of research on the subject. Steve August, a physiotherapist in New Zealand, is the only person in the world who is having consistent success treating this condition. It is likely because he had it for 7 years because of a rock-climbing accident and was desperate to find a solution. Here’s what worked best for me after 3 years of trial, error, and assiduous and desperate research.

Exercise: Backpod in hooklying
- Stage 1: 15 minutes with 3 pillows 1 week 1x a day, at 2 weeks reduce to 2 pillows, at 3 weeks reduce to 1 pillow.
- Stage 2: As this activity becomes a bit less tender or difficult try lifting your arms over your head as you take a deep breath in, then bringing your arms back down to your side as you exhale. Try 10 x.
- Stage 3: Try this on all regions of the thoracic spine- the upper, middle, and lower regions.
Logic: Shift facet joints thoracic spine posteriorly indirectly and improve breathing capacity almost immediately. The ribs also slide posteriorly by leveraging the spinous process’ anteriorly and inferiorly with an anterior force from an extremely firm carbon fiber device (backpod). Thus, the biomechanics of the ribs and the posterior rib joints and thoracic spine facet joints are realigned such that the anterior rib joints don’t have to move excessively and feed into this chronic inflammation.
Note: There is no substitute for this device; a foam roller or another object you have around your house will not produce the same results. When using the Backpod, you may experience tenderness: it is extremely strong and hard on purpose. If you are in the recent injury phase, usually up to 3 days after re-injury (acute inflammation), almost anything you try will fail. You should first address the inflammation with medicines, icing, resting, and avoiding re-injury activities. (Steve August) https://www.bodystance.co.nz/en/costochondritis

Exercise: 30 to 80 degrees shoulder abduction with shoulder blades on wall and arms on wall with lower trapezius muscle activation for scapular upward rotation
Instructions: Shoulder blades back, head upright, try and flatten midback into wall, create movement of arms upward on wall with lower trapezius muscles activation. To do this squeeze lower should blades together. Try to inhale with lateral rib cage on both sides when you are lifting arms, exhale with arms coming back down. Upon end of exhalation there should be a relief of spasms of rib cage.
Frequency: 5 x repeat, 2 x a day, 5 x a week, 6 weeks
Logic: Activation lower trapezius and other upward shoulder scapular rotators to help give space for lateral rib cage movement in posterior chest wall region. (Theory only) It seems to free up thoracolumbar fascia and fascia around rib cage.
Note: Create upward arms movement like picture with shoulders against wall. Go from about 30 to 80 degrees upward. Create movement with mid-back (lower trapezius muscles) by squeezing shoulder blades a bit together. (Scibek, et al.)
Exercise: Anterior pelvic tilt and activation multifidus/erector spinae. Roll pelvis forward, arch and extend mid back. Think opposite of rounded kyphotic back. (Takaki, et al.)
Frequency: Try to hold for 10 seconds 5 x, 3 x a day, 5 x a week, 6 weeks
Logic: Hold facet joints in place posteriorly with mid back and low back muscles
Note: Try and keep shoulders back, chest out, mid back region back and not rounding shoulders forward…and feel mid back muscles activated.
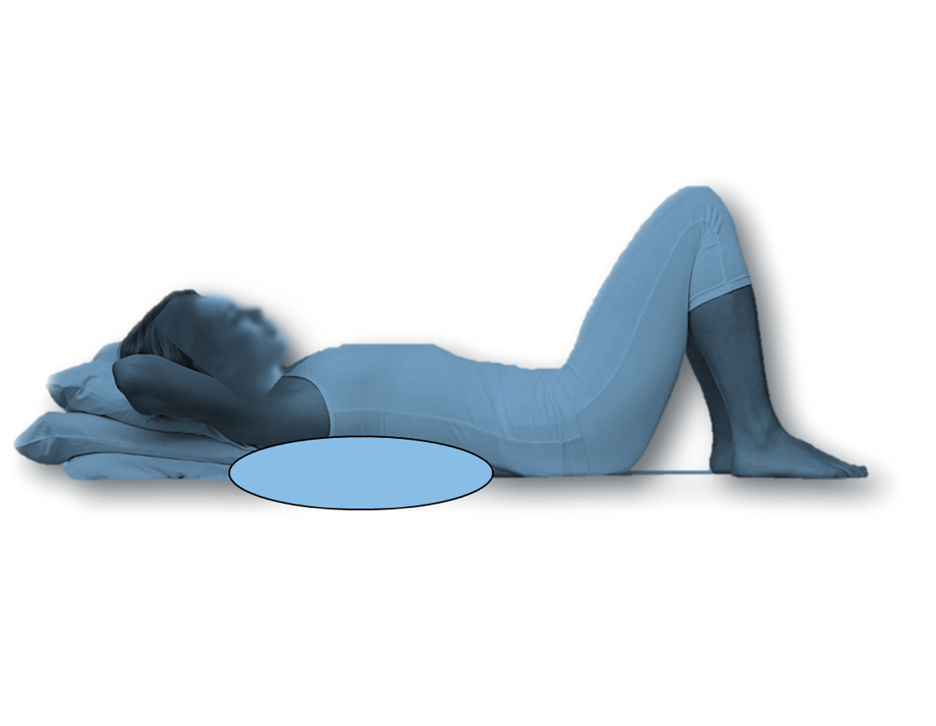
Exercise: Lying down with pillow under midback
Frequency: 6 weeks, 15 minutes at a time. If you can sleep like this—wonderful! Be careful to have some support for your neck.
Logic: Helping rib cage stay open with breathing and not become as stiff in the thoracic spine region. It allows rib cage to relax as well. After a few minutes you should feel your breathing come back to “normal” and less tight and painful in the rib cage. It lasts after getting up for about an hour.
These treatments can make a profound impact on the lives of your patients. I truly believe that this information is the only information available globally that can help current costochondritis patients consistently, aside from that pioneerd by Steve August. Ask any physician has seen patients with this condition. Those in the medical community continue to struggle to find effective treatments for this condition. Notice there is no treatment addressing bracing around the whole rib cage. It can cause pneumonia, decreased vital capacity, and shortening of the intercostal muscles and fascia for many years.
CITATIONS
- August, Steve. Costochondritis. The Backpod. https://buybackpod.com/pages/costochondritis
- Mott, et al. “Costochondritis: Rapid Evidence Review.” South Baldwin Regional Medical Center Family Medicine Residency Program, Foley, Alabama.
- Proulx, et al. “Costochondritis: Diagnosis and Treatment.” American Family Physician, vol. 80, no. 6, 2009, pp. 617-620.
- Scibek, JS, and Carcia CR. “Assessment of Scapulohumeral Rhythm for Scapular Plane Shoulder Elevation Using a Modified Digital Inclinometer.” World Journal of Orthopedics, vol. 3, no. 6, 2012, pp. 87-94.
- Sinhorim, L., et al. “Potential Nociceptive Role of the Thoracolumbar Fascia: A Scope Review Involving In Vivo and Ex Vivo Studies.” Journal of Clinical Medicine, vol. 10, no. 19, 2021, p. 4342.
- STEADI_ClinicianFactSheet-a.pdf. Centers for Disease Control and Prevention (CDC), www.cdc.gov.
- Takaki, et al. “Analysis of Muscle Activity During Active Pelvic Tilting in Sagittal Plane.” Physical Therapy Research, vol. 19, no. 1, 2016, pp. 50-57.
- Qureshi, I., et al. “Rib Fracture Management in Older Adults: A Scoping Review.” Brown Hospital Medicine, vol. 2, no. 3, 2023.
Disclaimer: This article is presented for educational purposes only and should not be interpreted as medical advice. Always consult with your physician or a qualified healthcare provider regarding any medical concerns or conditions.