Using the Transtheoretical Model to Encourage Patient Independence

By John Huller, PT, DPT, CSCS
Geriatric Clinical Resident
NJ South
As skilled clinicians across our respective disciplines, we engage with our patients on not only a professional level but typically also by exploring their personal lives, family history, and individual idiosyncrasies. As soon as we pull up to a patient’s home, we begin to collect data on everything related to their prospective plan of care (home environment, caregiver assistance, tidiness, prior level of function, etc.). This information helps us determine many prognostic factors on top of whatever physical impairments we also discover along the way.
By happenstance, our goal is to almost never see our patients again, as this will typically indicate they are functionally healthy and no longer in need of our services. Yet, we still encounter “frequent fliers” and at times have a quick patient turnaround, which ultimately indicates a relapse in function. Where did we go wrong? They were doing so well in therapy!
Unfortunately, most adults are generally sedentary, and ~50% of those who join an exercise program will drop out within 3-6 months. Older adults specifically are the largest segment of sedentary adults; with an excess of 8.5 hours/day sitting. This increased risk of chronic disease, frailty, loss of function, and social isolation cannot be understated. Although our services may provide the CDC-recommended weekly exercise guidelines, after we leave that door, we know about half of the time those individuals will not continue on their own. So the question then becomes, what can we be doing better?
What is the Transtheoretical Model?
The transtheoretical model (TTM) was originally developed with a focus on smoking cessation but has also been researched and applied to weight management, physical activity/exercise, and either adding (positive) or removing (negative) habitual behaviors. The TTM incorporates various schools of thought which allow for the most effective techniques to that specific individual, at their specific stage.
As with many pathology-related guidelines and CPRs, the stages of change (SOC) are dynamic in nature, with the ability to quickly shift from one stage to the next. As with everything in life, nothing’s perfect, and non-compliance/relapses are to be expected. It’s how we intervene after the fact to prevent patient relapses from occurring in the future.
Yes, there are always legitimate reasons that could account for relapses in function (falls, illness, or hospitalizations), but more often than not it’s a poor carryover with health/wellness management. Our home exercise programs suddenly get “lost” and that walker turns into an oversized clothes hanger.
The three most important factors in TTM involve the patient’s self-efficacy, decisional balance, and processes of change utilized. Essentially, this breaks down to how does the patient see themselves, how do they see the benefits of change, and how do they modify their thoughts, feelings, and behaviors?
Speech-language pathologists are much better equipped for utilizing these practices in relation to cognitive therapy. However, occupational therapists, and to an even lesser extent, physical therapists, do not nearly get enough training about incorporating these into practice. The TTM can help therapists identify what SOC someone may be in and then alter exercise and education intervention to optimize delivery and efficiency of care.
Incorporating TTM Into Clinical Care
Our skilled care requires us to not only individually tailor treatments, but also remain adaptable as patient’s situations may change. One area that can be underutilized at times is in relation to psychosocial interventions. We are all excellent at addressing those physical needs; but what are we doing that can help facilitate prolonging patient success after they are inevitably discharged? One of the most prominent ideas in research is the TTM and SOC.
And while we cannot bill insurance as if we were licensed psychologists or counselors, we can incorporate these theories into our own practice.
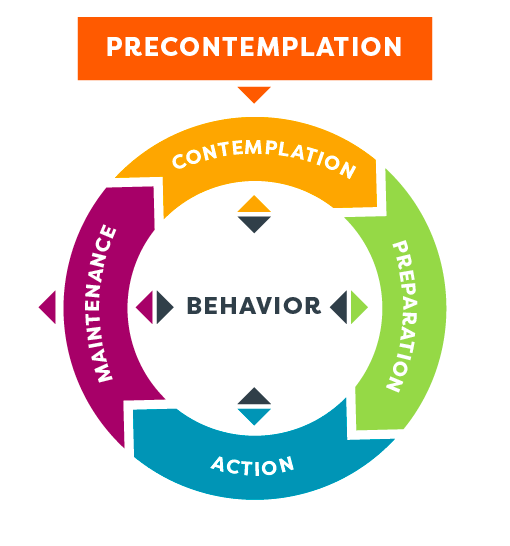
5 Official SOC:
- Precontemplation – build awareness for my need to change
- Contemplation – increase my pros for change and decrease my cons
- Preparation – commit and plan
- Action – implement and revise my plan
- Maintenance – integrate change into my lifestyle
Benefits of TTM for Older Adults
Research has shown a significant difference in depression and QOL among community-dwelling older adults when combining behavioral and exercise programs in tandem, compared to exercise alone. Additionally, it has even been shown to reduce low back pain, improve back muscle endurance and enhance physical function, compared to non-TTM usage.
The interactions between processes used within interventions of TTM are shown to be associated with increased compliance with moderate physical activity within the general population. In-person education within sessions has been shown to produce the most significant results compared to simply giving print/digital handouts.
The most encouraging statistic noted with physical activity is that the most pronounced changes in individuals occur between pre-contemplation-contemplation and preparation-action. Therefore, those who may not currently be set up to change will have the greatest benefits out of any of our patients.
Our patients thrive on human interaction, well at least most do. It is what is key to transitioning a patient to want to change and in a post-COVID world where telehealth still remains a dominant form of healthcare services, we are set up to really make a difference in our patients’ lives.
How Clinicians Can Incorporate TTM
It is important to build a “strong therapeutic alliance” with our patients as seen also in the fields of psychotherapy and nursing. Body language is key to establishing this relationship through eye gaze, head nodding, and smiling. Now since we’re all behind masks, that last one can be a bit tricky but I think you get the point. Feedback such as forward-leaning and touch are also key factors to helping establish trust and allow patients to see our attentiveness.
It is important to consider not only what is said, but also the manner in which it is conveyed. Just think of all those spirited discussions you may have had in your own personal lives that could have been avoided with an eye wink every now and again. These affective behaviors are valued by our patients and help establish both trust and confidence with us.
As clinicians, we can guide patients through all of these factors and help them grow in confidence as they improve in function. We can raise their awareness of chronic disease management through education, explaining handouts, and using visual graphs to appeal to their learning style. We want to avoid our education packets becoming the stereotypical travel brochure in the junk drawer.
For the more difficult patients, we should not be afraid to be a little dramatic in the consequences to their health if they do not follow a skilled plan of care. On top of our progress reports, we should have patients self-reflect on their improved confidence or perceived reaction to interventions. We do this somewhat with the PSFS but don’t forget to incorporate more specific measures such as LEFS, Oswestry, Brief Fatigue index, Quick Dash, etc.
When it comes to environmental changes and decreasing caregiver burden, we usually do a particularly good job in terms of readiness to change and home safety assessments. We also should encourage individuals towards a healthier lifestyle by explaining to them the reasoning behind our FOM selections and when normative values are available use these as a guide to help them self-motivate.
The use of self-liberation and saying affirmations out loud can assist patients in making and believing in that commitment to exercise regularly. When outside support is available, try to actively engage family/friends as part of the therapy sessions to assist in modifying the behavior. In some cases maybe removing the caregivers actively from treatment could improve compliance as well. With today’s technology, we can really start to leverage smart devices to encourage activity with reminders/alarms set for exercise as well. If Alexa and Google are already listening to our sessions anyway, we might as well use them!
You May Already Be Using TTM
Although the TTM may seem at times very dense, we are already using it in our day-to-day practice, just not as efficiently as we may be able to. One recommendation specifically for those who may be interested in learning more involves the self-help book Changeology. Written by one of the co-founders of TTM, it can not only help guide you, but also your patient’s into a better understanding of their behavior decisions in relation to all aspects of life, not only health.
We should always be on the lookout to change our patients’ lives for the better and utilize TTM as another tool in your toolbox. Greek philosopher Heraclitus once said, “The only constant in life is change”, we might as well get used to managing it as best we can.