Addressing Pelvic Floor Concerns for Patients With Urinary Incontinence Issues

By Katie Butcher, OTR/L
Occupational Therapist
As experts at analyzing the physical, emotional, spiritual, and mental aspects of a patient, occupational therapists can identify all the barriers that might exist for their patients. When creating an occupational profile of a patient, OTs automatically consider how their habits, roles, and routines might impact their functional deficits.
Since approximately 40% of the older adult population have urinary incontinence (UI) issues, this topic is likely to come up in discussions with our patients. The issue impacts their quality of life and will likely be an area of concern when completing occupations such as toileting, sexual activity, dressing, and the functional mobility of getting to the bathroom in time.
OTs can address UI and pelvic floor issues when completing the patient’s occupational profile by evaluating their physical presentation along with the environment and social contexts. OTs often focus on a patient’s general positioning and alignment throughout the body in both sitting (especially on the toilet) and standing. For example, many older adults benefit from durable medical equipment for the toilet that raises the height of the seat which increases their safety. However, this puts their hips below 90 degrees of flexion, potentially making it difficult to pass stool or urinate. It’s best to avoid semi-squatting on the toilet because it prevents the pelvic floor from relaxing around the urethra which can impact the rate of prolapse.
Optimal posture would be to maintain a natural lumbar curve (not slumped over) and to not lean forward at the hips. Knees should be wide apart on the floor to increase their base of support.
6 OT Bathroom Tips for Older Patients With Pelvic Health Issues
Throughout the intervention, OTs can include pelvic floor education and precautions and how they relate to the occupation of patients. Below are some examples of education that could positively affect a patient’s habits, roles, and routines.
Staying Hydrated
Many patients say they withhold their water intake so they “don’t have to go to the bathroom all day long” but this may actually compound their issue. If a patient isn’t drinking enough water, their pelvic floor becomes more acidic, which can cause damage to the brain and bladder neural connection.
- Recommend drinking half your body weight in fluid ounces. This may seem daunting, so it is advisable to start with a smaller goal of drinking eight glasses of water a day.
- Advise patients to sip water instead of gulping so that the body has time to fully filter and process it. The body will still expel the water even in a dehydrated state before it is filtered and processed.
- Caution drinking excess coffee or alcohol. Because of the acidity of coffee, it’s best to drink fewer than three cups a day.
- Alcohol is a diuretic that is also dehydrating, so it’s best to limit excessive intake.
Limit “Just in Case” Bathroom Trips
This tends to disrupt the brain and bladder connection of sensing when one truly has to urinate. A healthy bladder usually voids urine five to eight times a day. For those 60 years of age or older, it’s typical to get up to urinate once or twice a night.
Night-time urination is a sympathetic activity, meaning it is crucial to maintain this so there is relaxation and contraction of the urethral sphincter to help stop urine output. This is why it is not the time to “withhold” but to instead focus on training with a more consistent urination schedule during the day until the brain to bladder connection normalizes.
Don’t Strain to Urinate
Educate patients to breathe and relax during their toileting routine. This shouldn’t require any effort. There might be some hypertonicity if there is an effort with urination — like wringing out a wet washcloth. Urine flow should be relatively consistent. Constipation or backed-up stool can be the number one cause of frequency and urgency.
Don’t Rush to the Bathroom
This can lead to falls by increasing the autonomic nervous system and removing the focus on safety precautions. Advise your patient to sit or stand for a minute and see if the symptom calms down after a minute of breathing.
- Urinating every two to four hours is optimal. Sometimes advising patients to note when and how often they are going to the bathroom can offer helpful information.
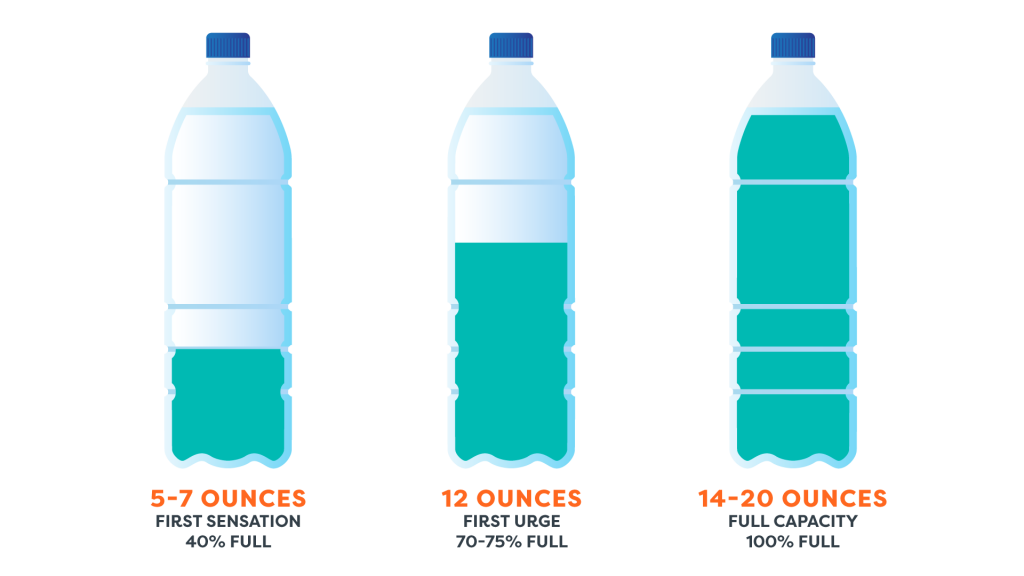
- Depending on how much time it takes a patient to get to the bathroom and gather necessary supplies, having them make a plan for when they first sense urgency and to take their time. Orient a patient to the image provided below and have them think about what their intake was like before the sense of urgency.
Focus on Breath Patterns Throughout the Day
The diaphragm plays a large role in supporting and working with the pelvic floor. Withholding one’s breath when reaching, bending for objects, performing exercises, or even periodically throughout the day can put pressure on the pelvic floor muscles whose one of several jobs is to protect our organs!
Embed some type of relaxation or breathing exercise as a part of one’s home exercise plan. To help with HEP adherence, schedule relaxation activities for the nervous system using task analysis. Include activities such as:
- Pool exercises/swimming
- Yoga
- Meditation
- Self-care (hair, nails, face mask)
- Chewing gum or humming
- Gargling (anything repetitive and rhythmic spent throughout the day)
- Boxed breathing, nostril breathing, or diaphragmatic breathing
Relax
If incontinence is a vocalized concern of the patient or is relevant to your plan of care, teach them that relaxing the pelvic floor is equally important as contracting or performing a “Kegel.” Keep in mind that:
- It’s as important to relax as it is to contract. The same can be said about the bicep or any other muscle. If a bicep is constantly in a concentric contraction, then the eccentric contraction and relaxation are that much more difficult. You can’t address muscular dysfunction without full ROM.
- Not everyone knows how to properly Kegel let alone how to reverse Kegel. When the muscles of the pelvic floor slowly lift up from the center of the pelvis and anus, some people describe it as gently drawing up your urethra. The patient shouldn’t feel any pressure.
Occupational Therapists Can Make Patients’ Lives Easier
With adequate education, any practitioner can become competent in addressing pelvic floor-related issues. It is an OT’s job to make every patient feel safe and comfortable bringing up these concerns and to help them address them. Issues related to incontinence, prolapse, or any other pelvic floor-related issue can create occupational barriers for a patient, and OTs are charged with helping to break down those barriers. OTs should make appropriate referrals for patients by reaching out to team members and colleagues for recommendations of providers in your local area.